
Research Article | DOI: https://doi.org/10.31579/2693-7247/010
1Department of Pediatrics, Schulich School of Medicine & Dentistry, London, ON, Canada N6A 5W9
2Instituto Nacional de Pediatría, México City, México 04530
3Universidad Nacional Autónoma de México, México City, Mexico 04510
4The Hospital for Sick Children. University of Toronto. Toronto, ON, Canada M5G 1X8
5Laboratorio de Investigación en Nefrología, Hospital Infantil de México Federico Gómez, Mexico City, Mexico 067210.
6Departments of Medicine and Pathology and Laboratory Medicine, Schulich School of Medicine &
Dentistry, University of Western Ontario, London, Ontario, Canada N5A 5A5
7Lilibeth Caberto Kidney Clinical Research Unit, London Health Sciences Centre; and Department of
Medicine, Schulich School of Medicine & Dentistry, University of Western Ontario, London, ON, Canada N6A 5W9
8Children’s Health Research Institute, University of Western Ontario, London, Ontario, Canada, N6C 2V5
*Corresponding Author: Carmen Inés Rodríguez Cuéllar, Pediatric Nephrologist Department of Pediatrics, Fundación Clínica Shaio Bogotá, Colombia.
Citation: Rodriguez Cuellar CI, Alvarez-Elías AC, Elisa C. Yoo, and Filler G, (2020) Only Modest Effect of Lipids and Albumin on Apparent Mycophenolic Acid Clearance in Pediatric Transplant Recipient – a Retrospective Cohort Study. J Pharmaceutics and Pharmacology Research 3(4); DOI:10.31579/2693-7247/010
Copyright: © 2020, Carmen Inés Rodríguez Cuéllar, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 August 2020 | Accepted: 03 September 2020 | Published: 23 December 2020
Keywords: kidney transplantation, pediatric, mycophenolate mofetil, apparent total clearance, bioavailability
Background: There is growing evidence for the need of therapeutic drug monitoring (TDM) of the active compound Mycophenolic Acid (MPA) of mycophenolate mofetil therapy for the management of antirejection therapy after pediatric renal transplantation. While there is substantial inter- and intra-patient variability of MPA exposure, the factors affecting its apparent clearance (CL/F) are understudied. The objective of this study was to determine the relationship between MPA CL/F, eGFR, creatinine, Cystatin C, triglycerides, cholesterol and albumin.
Material and Methods: We calculated 1004 estimated mass-spectrometry-determined MPA CL/F using trough concentrations from 35 pediatric renal transplant patients.
Results: Mean age was 8.7±4.6 years at transplant with a median follow-up of 5.8 years. Each patient had a median of 30 MPA trough concentrations. The median MPA AUC was 53.21 mg*h/L, the median CL/F was 8.66 L/h. Univariate and multivariate analysis revealed significant correlations of CL/F with creatinine, triglycerides, cholesterol and albumin, and very weakly with hemoglobin, whereas cystatin C was unrelated. Especially higher lipid levels and weekly, but significantly, lower albumin augmented CL/F. However, the correlations were not strong enough to predict CL/F.
Conclusion: The data presented indicate the necessity for MPA TDM and suggest that dose modifications may apply in the face of low serum albumin and hyperlipidemia.
In the setting of pediatric renal transplantation, critical dose drugs such as calcineurin inhibitors, and inhibitors of the mammalian target of rapamycin (MTOR), require therapeutic drug monitoring (TDM) [1]. The need for the TDM of mycophenolate mofetil (MMF) has been debated [2]. Early after renal transplantation, there is growing evidence that TDM of the active compound of MMF, mycophenolic acid (MPA), may help reduce underexposure and allow maintenance of the target exposure area-under-the-time concentration curve (AUC) of 30-60 mg*h/L may reduce rejection [3-5]. There is less evidence for the benefit of long-term MPA monitoring after transplantation, even though the trough level may be a feasible biomarker of exposure when looking at a fixed combination of tacrolimus and MMF [6]. Some recent evidence suggests that long-term MPA underexposure may be related to the formation of de novo donor-specific antibodies (DSA) [7, 9], which are associated with inferior graft outcomes [10, 11]. MPA exposure may be more variable than that of calcineurin inhibitors [2]. Age and drug interactions clearly affect the pharmacokinetics in pediatric renal transplant recipients [12, 13]. However, TDM of MPA is not widely available, and many centers do not routinely measure MPA levels. In a few early adult publications on the pharmacokinetics of MMF, it was suggested that hemoglobin, albumin and GFR affect the MPA clearance [14-16]. We are unaware of any studies regarding the impact of changes in hemoglobin, albumin or GFR on the MPA exposure in pediatric renal transplant recipients. We therefore embarked on a retrospective analysis of all available MPA trough levels in our long-term pediatric renal transplant cohort who only received concomitant tacrolimus. We calculated the apparent clearance (CL/F) from an estimated AUC based on published literature [6]. It was hypothesized that serum creatinine, cystatin C, eGFR, albumin, and hemoglobin would contribute to the variability of CL/F. Moreover, we also included cholesterol and triglycerides. In addition to testing for UGT1A9 gene polymorphispms, knowledge of these interactions might guide clinicians who do not have access to MPA TDM to adjust MMF dosing. To study the impact, we used correlation analysis between the proposed factors and the apparent MPA CL/F. We hypothesized that higher triglycerides and higher cholesterol and lower albumin may enhance MPA CL/F.
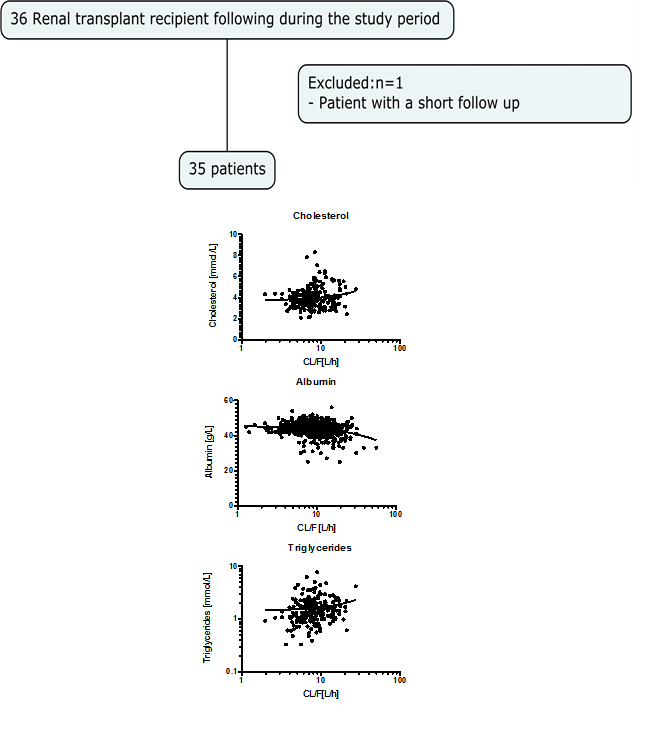
The study was approved by the Western University Research Ethics Board (HSREB File Number 105148). [6, 7, 12, 13] We retrospectively analyzed all existing data on 35 pediatric renal transplant recipients who were followed between January 1st, 2004, and June 30th, 2018. This study cohort included all pediatric patients who had undergone renal transplantation <18 n=2),>
Gender, age at transplant, follow-up time after transplantation, daily concomitant medication (data not shown), and anthropometric data (height, weight, blood pressure) were obtained from the patient’s paper and electronic charts. Along with all available MPA concentrations, we used our electronic health record to obtain the following laboratory tests: cystatin C concentration, creatinine, albumin, hemoglobin, and cholesterol and triglyceride concentrations. None of the patients had elevated transaminases or elevated bilirubin. eGFR was calculated using the Filler formula [18]. AUC was calculated from the trough level using the formula:
AUC = 6.743 x Ctrough + 34.8 [6]
where Ctrough is the pre-dose trough level of MPA.
CL/F was calculated using the Dose for a dosing interval divided by the AUC using the formula:
CL/F = Dose/AUC
MPA and tacrolimus concentration measurements and adjustments
All patients were treated with MMF with concomitant tacrolimus. Tacrolimus was started at 0.15 mg/kg/dose and modified according to the patient’s trough concentrations. While not subject to this study, target tacrolimus concentrations were 10-20 ng/mL in the first month post-transplantation, followed by a gradual decrease of the trough concentration to 5-10 ng/mL at one year and 4-6 ng/mL thereafter. The reason for exclusively using patients with concomitant tacrolimus was the fact that the MPA pre-dose trough level could be used as a surrogate for the MPA area-under-the-time-concentration curve [6]. Data were only included until the 18th birthday.
Patients started on 1200 mg of MMF per 1 m2 body surface area in 2 divided doses [19]. A higher starting dose was occasionally chosen for small children. Doses were adjusted to the nearest 250 mg to make dosing more convenient in case they took the medication in the form of capsules. Dosing was individually adjusted based on MPA trough concentrations that were measured during the patients’ routine clinic appointments. Although physicians generally aimed to maintain an MPA trough concentration >1.3 mg/L [7], the target exposure varied between physicians and patients. For instance, a lower MPA exposure was typically targeted in patients with BK virus nephropathy or leukopenia, though there was no formal protocol to this effect.
MPA concentrations were measured with HPLC/MS/MS. The lower limit of quantification for the MPA concentrations was 0.1 mg/L. For the estimation of creatinine-based eGFR, we used the new Schwartz formula [20]. The cystatin C eGFR was calculated using the formula proposed by Filler and Lepage [18]. The total imprecision for all tests was less than 5%.
Data were tested for normality using the D’Agostini Pearson Omnibus test. Descriptive data are represented as mean ± one standard deviation (for normal distribution) or as median and interquartile range (for non-normal distribution). As most parameters were not normally distributed, we used Spearman rank correlation tests to determine which parameters correlated with CL/F in a univariate approach. No adjustments were made for missing values. This was followed by mixed effect multivariate regression analysis, because of the interdependencies of several factors.
All analyses were performed using Excel (Office for Mac 2011, version 14.3.8), Graph Pad Prism for Mac OS X version 5 (Graph Pad Software, San Diego, CA, USA) and STATA version 11.2 for Mac (StataCorp, College Station, TX, USA). A p-value <0>
The demographic characteristics of the cohort are described in Table 1.
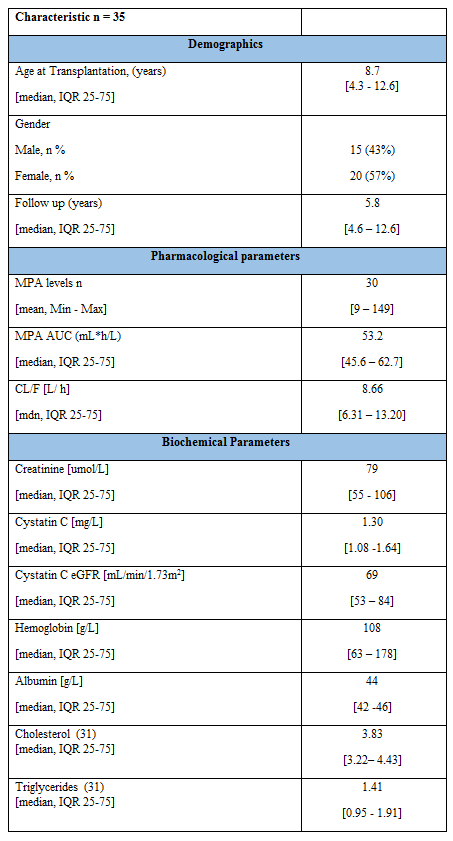
Thirty-five patients were included, 20 of whom were female. The underlying diagnoses were: renal dysplasia n=10, obstructive uropathy n=11, FSGS n=4, ARPDK n=3, glomerulonephritis n=2, spina bifida n=2, cystinosis n=1, HUS n=1, hyperoxaluria type I n=1. The mean age at transplant was 8.7±4.6 years, with a mean follow-up of 7.8±4.8 years (median 5.8 years, 25th percentile 4.6, 75th percentile 12.6 years). Each patient had a median of 30 MPA trough concentrations (range 9-149). From the 1138 MPA levels, we could calculate 1133 MPA AUCs, and 1005 CL/F. The median AUC was 53.21 mg*h/L, with a 25th percentile of 45.59 and a 75th percentile of 62.72 mg*h/L. Median CL/F was 8.66 L/h with an interquartile range from 6.31 to 13.20 L/kg, which means 70-fold variation.

We then performed correlation studies. The results are provided in Table 2 for the CL/F based on dose/kg. In the univariate analysis, creatinine, albumin, cholesterol and triglycerides all correlated significantly with CL/F [L/h] (table 2), whereas cystatin C,
cystatin C eGFR, and hemoglobin did not. The correlations between CL/F and albumin, cholesterol and triglycerides as well as the non-linear regression lines are provided in figure 1.
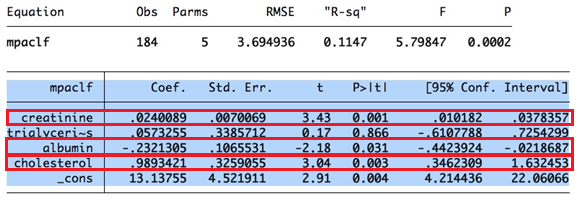
Finally, we performed mixed effect multivariate regression analysis for CL/F [L/h] on all available observations. Only creatinine, albumin and cholesterol remained significant in the multiple logistic regression analysis (table 3). Triglycerides no longer remained significant.
In this retrospective cohort study, we had 1138 MPA levels of 35 renal transplant recipients, for which we could calculate CL/F. We had a median of 30 MPA CL/F values with a median follow-up of 5.8 years. In this sizeable cohort, we found 50% of the estimated AUC between 45 and 62 mg*h/L, which is well within the expected range [2]. The median CL/F was 8.66L/h, which is also comparable to that in the literature [21]. In the literature, CL/F was expressed as mean of 11.7±7.0 L/h, whereas the mean was 10.19±5.6 L/h in our cohort. This difference was not significantly different from Jaqcz Aigrain [21]. Using univariate correlation analysis, MPA CL/F correlated with creatinine, albumin, cholesterol and triglycerides. The lack of correlation with estimated GFR and cystatin C was unexpected. As cystatin C is a better marker of GFR in children than creatinine [22], the impact of GFR on the MPA clearance is probably not very important. Using mixed model regression multivariate analysis, CL/F was still independently affected by creatinine, albumin and cholesterol. It should be highlighted that these findings were only correlating modestly and may not be of high clinical importance. Nonetheless, they point to increased MPA clearance in the setting of hypoalbuminemia and hyperlipidemia, which the physician needs to be aware of, especially if no MPA monitoring is performed.
To explain these findings, a review of the pharmacological properties and elimination of MMF is necessary [15]. MMF is a prodrug of MPA that rapidly converts to MPA by first pass metabolism in the liver [23, 24]. Its volume of distribution is largely due to the plasma volume (99.99%), where the drug is heavily bound to serum albumin, in patients with normal renal and liver function [15]. Binding of MPA to albumin is constant over a wide measurement range [25]. Unfortunately, without measurement of free MPA levels, we cannot assess the MPA plasma protein binding, but it is conceivable that the availability of albumin affects the amount of unbound MPA and thus alters the clearance [15]. Ninety-three of main metabolite, MPA-G, is recovered in the urine while 6% is recovered in feces. Excretion of MPA-G in the urine is believed to be mainly via active tubular secretion [26].
Similar to adult patients, we found an effect of serum albumin in the CL/F of MPA [26] de Winter et al. described an association between albumin concentrations total MPA while the unbound MPA remains unaffected [27]. We do not have free MPA levels, but our findings would be in agreement with the data from adults which suggest that hypoalbuminemia causes an increase the clearance of MPA [26].
As far as we are aware, the impact of triglycerides and cholesterol on MPA clearance has not been reported previously in pediatric patients. We only found one report in adults [28]. The herein reported moderate positive impact of triglycerides on MPA CL/F is in keeping with a recent paper by Vial et al that described a displacement of drugs from plasma protein binding via competition or allosteric modulation [29]. The previously reported impact of very low albumin on MPA clearance may in fact be more due to the secondary hypertriglyceridemia induced hypoalbuminemia. Vial et al. report 2.2-fold increase of MPA CL/F when the molar ratio of fatty acid/albumin increases to 5:1 which would resemble significant hypertriglyceridemia [29].
Our study has several limitations. The retrospective nature of the study forms a significant limitation. However, such a large number of CL/F measurements would not be easily obtained in prospective studies. The lack of complete pharmacokinetic profiles is a shortcoming. However, as shown in our previous work, MPA trough levels resemble a reasonable surrogate of the AUC when they only have concomitant tacrolimus [6]. In fact, our estimated AUCs compare very well with reported AUCs. We only included the measurements with HPLC/MS/MS. It is known that EMIT may lead to overestimation of MPA levels [17]. As this was not a planned study, there is wide variability of the number studies regarding albumin, hemoglobin and lipids in these patients. This clearly limits the power of the multivariate analysis. Especially due to the low number of lipid studies. The importance of measuring lipids in the patients has recently been recognized [30]. Nonetheless, the large number of CL/F measurements forms a considerable strength.
The current study highlights the moderate impact of MPA CL/F with hypoalbuminemia and elevated cholesterol which enhance the MPA CL/F. Transplant physicians looking after pediatric renal transplant recipients need to be aware of these phenomena and may consider increasing the MMF doses in the setting of hypoalbuminemia or significantly elevated cholesterol. Intuitively, pediatric renal transplant recipients receive lower MMF doses in renal failure, whereas it is the impression that the impact of hypercholesterolemia and hypoalbuminemia are not used for dose adjustments. Ideally, TDM if MPA levels (including unbound MPA) is performed, but in the absence of available levels, physicians should consider the enhanced clearance for MMF dose adjustment.
All authors had no relationships or circumstances that present a potential conflict of interest.
Conflicts of interest and funding sources: None.
We want to acknowledge the staff of the laboratory at London Health Sciences Centre for their excellent and high precise analytical work.
GF conceived the study, applied for the ethics submission, was involved in all aspects of the paper generation and revised each draft, performed the statistical analysis, and coordinated all coauthors’ activities. GF and CR performed the statistical analysis, interpreted the data and wrote the first draft. CR and EY collected and interpreted the data. ACA provided critical input into all aspects of the design and execution of the study and participated in all phases of the paper writing. All authors participated in revising the manuscript critically for important intellectual content and approved the final version to be submitted to the journal.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
